

Quick Answer: Longer than most people do, but not indefinitely. Antidepressants need several weeks at a therapeutic dose before you can fairly judge whether they're working, and side effects usually show up before benefits do. Your prescriber will have a specific review point in mind. What matters is that the trial is long enough, at a high enough dose, taken consistently, because those three things are what make it count as a real trial rather than an inconclusive one. Most people either stop too early or wait far too long. Stopping at two weeks because nothing has changed means you never find out whether the medication would have worked. Staying on something for two years because it's "probably doing something" costs you the same time in a different way. This post covers what should happen in the early weeks, what makes a trial count, and why keeping a record of it matters more than you'd expect. Why it takes weeks rather than days Antidepressants change neurotransmitter levels fairly quickly, but the downstream changes that actually shift mood take longer to develop. That gap is why the first stretch on a new medication can feel like the worst of both worlds: you're getting the side effects without any of the benefit. This isn't the medication failing. It's the normal shape of the thing. Knowing that in advance is the single best predictor of whether someone sticks with a trial long enough to learn anything from it. Improvement is also usually gradual rather than sudden. People often notice it first in sleep, appetite, or energy, and only later in mood. Sometimes the people around you notice before you do. What should happen in the first few weeks? Expect side effects early. Nausea, headaches, restlessness, changes to sleep, and digestive upset are common at the start and often ease as your body adjusts . Your prescriber can tell you which ones are expected to settle and which ones aren't. When to call sooner rather than waiting it out: Your mood gets noticeably worse rather than better New or increasing agitation, restlessness, or inability to sit still New or worsening thoughts of harming yourself Any side effect that's severe, or that you can't function around A rash, or anything that feels like a physical reaction rather than an adjustment None of these are reasons to be stoic. Early worsening is uncommon but it's real, and it's specifically why prescribers want to see you sooner after a start or a dose change rather than later. If you're having thoughts of harming yourself, call or text 988, or go to your nearest emergency department. Don't wait for your next appointment. Don't stop a medication abruptly on your own either. Several antidepressants cause discontinuation symptoms if stopped suddenly, and those get mistaken for relapse. If you want off it, tell your prescriber that and they'll taper you. What actually counts as an adequate trial Three things have to be true before a medication trial tells you anything useful: A therapeutic dose. Many people are titrated up gradually and then stay at a starting dose that was never meant to be the destination. A trial at the lowest dose isn't a failed trial. It's an incomplete one. Enough time at that dose. The clock starts when you reach the therapeutic dose, not when you first took the tablet. This is where a lot of "failed" trials fall apart on review. Consistent use. Missed doses, stopping and restarting, or gaps caused by cost or pharmacy issues all muddy the result. Say so honestly at your review appointment. Prescribers are not shocked by this, and it changes what they recommend. If any of the three is missing, the honest answer is that you don't yet know whether the medication works for you.

Quick Answer: They do different jobs. A therapist treats symptoms through structured talk therapy. A psychiatrist or psychiatric nurse practitioner diagnoses, prescribes medication, and oversees medical treatments like TMS and Spravato. For moderate to severe depression and for OCD, most people do best with both. Which one you start with depends on your symptoms and what you've already tried. The question usually comes up at a practical moment: you've decided to get help and you're looking at two categories of provider with overlapping titles, or you've been seeing one of them for a while and you're not getting better. The distinction matters more than it looks, particularly if you're heading toward treatments that require a specific kind of prescriber. Here's who does what, when you need both, and where our own program fits. What a therapist does Therapists deliver structured psychotherapy. Depending on their training, that might be cognitive behavioral therapy (CBT), exposure and response prevention (ERP) for OCD, or trauma-focused approaches like EMDR or prolonged exposure. Sessions are usually weekly and run about an hour. Therapists in Ohio don't prescribe medication. That's the clean dividing line. What therapy is good at: changing the patterns that keep symptoms running, processing trauma, and building skills you keep after treatment ends. For OCD in particular, ERP isn't a nice-to-have alongside medication. It's a first-line treatment in its own right. What a psychiatrist does A psychiatrist is a medical doctor (MD or DO) who completed medical school, a psychiatric residency, and in many cases board certification. They diagnose, prescribe and manage medication, and oversee medical treatments including TMS and Spravato . Some psychiatrists also provide therapy, though many focus on medication and interventional treatment and work alongside therapists. A psychiatric nurse practitioner (PMHNP) is an advanced practice registered nurse with specialist psychiatric training who can evaluate, diagnose, and prescribe. In practice, a PMHNP working within a psychiatrist-led practice covers much of the same ground for straightforward medication management, with the medical director available for more complex cases. That's the model here: Dr. Mark Blair, MD , board-certified psychiatrist and Medical Director, with a psychiatric nurse practitioner providing medication management. When you need both For moderate to severe depression, combining medication with therapy generally works better than either on its own. They're doing different things. Medication addresses the biology; therapy addresses what you do with your days, your thinking, and your relationships. Neither substitutes for the other. For OCD, the standard combination is an SSRI plus ERP therapy. Medication alone tends to take the edge off without teaching you how to stop the compulsions. For PTSD, trauma-focused psychotherapy does the primary work, with medication supporting sleep, mood, and anxiety while you do it. If you're only seeing one and you've plateaued, adding the other is often the change that moves things, not another dose adjustment. Does it matter who prescribes? For a first antidepressant, often not much. Primary care physicians prescribe antidepressants routinely and are a perfectly reasonable place to start. It starts to matter in three situations: When treatment isn't working. Several failed medication trials is the point where diagnostic review by a psychiatric specialist adds something a routine refill appointment can't. When the diagnosis may be incomplete. Bipolar spectrum illness, OCD, and PTSD respond to different treatment than unipolar depression, and mistaking one for the other costs years. When you're moving toward interventional treatment. This is where credentials become a practical hurdle rather than a preference. TMS and Spravato both sit inside specific clinical and regulatory frameworks. Spravato can only be given at a certified treatment center under supervision, which is not something any prescriber can arrange. TMS is FDA-cleared for depression and covered by most major insurance plans when criteria are met , but those criteria include requirements around evaluation and oversight, and plans vary in how they define them. The practical consequence: if you've been told you don't qualify for TMS, it's worth finding out whether the reason was clinical or administrative. Those have very different fixes. A clinical exclusion means the treatment genuinely isn't appropriate for you. A documentation or credentialing issue means the treatment might be appropriate and the paperwork didn't support it. Ask which one it was, and bring that answer to your next consultation. At Optimum, TMS and Spravato are prescribed and overseen by a board-certified psychiatrist, and benefits are verified before you commit to anything .

Quick Answer: When antidepressants stop working, the next step usually isn't another prescription. It's a proper review of whether the medication was given a fair trial, followed by a conversation about treatments that work through a different mechanism entirely, like TMS or Spravato . For most insurers, a history of failed medication trials is exactly what qualifies you for those treatments. If you've been through several antidepressants over several years, you've probably had the same appointment more than once. A dose adjustment. A switch. An add-on. A few weeks of hope, then the slow realization that you're back where you started. At some point the question stops being "which medication next?" and becomes "is medication the right tool at all?" This post covers what actually happens when antidepressants stop working, what your prescriber should rule out first, and what the alternatives look like. What "stopped working" usually means Not all medication failure is the same thing, and the difference matters for what comes next. It never worked well enough. You took it as prescribed, at a therapeutic dose, for long enough, and your symptoms barely moved. This is the most common pattern in people who eventually look at TMS or Spravato. It worked, then faded. A medication that helped for months or years loses its effect. Sometimes a dose increase helps . Sometimes it doesn't, and the same thing happens with the next one. It worked partially. Your worst symptoms lifted, but you never got back to feeling like yourself. Partial response is easy to live with for years without ever calling it failure. You couldn't tolerate it. Weight gain, sexual side effects, blunting, fatigue. The medication may have been working, but the cost of taking it was too high. Each of these is a legitimate reason to look at something different. The third one in particular tends to go unnamed for a long time. What your prescriber should rule out first Before concluding that antidepressants have failed, a good psychiatric evaluation checks the boring explanations. This isn't stalling. It's the difference between changing treatment and changing treatment for the right reason. Was the dose and duration adequate? Antidepressants need several weeks at a therapeutic dose before you can judge them. A trial that was stopped early or never reached full dose is an incomplete trial, not a failed one. Is something else driving the symptoms? Thyroid problems, sleep apnea, chronic pain, alcohol use, and certain medications can all keep depression from lifting. Is the diagnosis complete? Bipolar spectrum illness, OCD, and untreated anxiety or trauma respond differently. Depression that isn't responding is sometimes depression that isn't the whole picture. Is anything getting in the way of consistent use? Cost, side effects, and missed doses all affect the result. If you've been through this review and the answer is still that the medications aren't working, you meet the working definition of treatment-resistant depression: an inadequate response to two or more adequate antidepressant trials. That label sounds discouraging. In practice it's the criterion that opens the door to treatments most insurers won't approve until you've reached it.

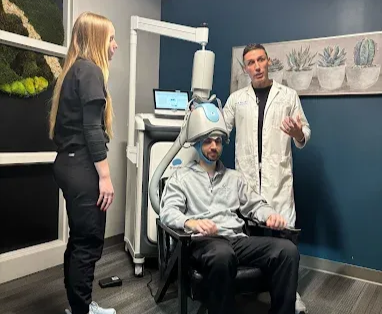
Quick Answer: TMS is a non-drug, non-invasive depression treatment that the FDA has cleared for use in adolescents as an add-on to therapy or medication. For most teens, the side effects are mild and temporary, and whether it's a fit is decided in a consultation - not from a web page. Below is what that clearance actually covers and what parents should ask. When a teenager has been through therapy and one or more antidepressants without much relief, families start looking for what comes next. TMS (transcranial magnetic stimulation) tends to come up quickly - and so does the question every parent types into Google first: is it actually safe for someone this young? This walks through what FDA clearance means, what the treatment involves day to day, and how to tell whether it's worth a conversation. What TMS actually is TMS uses focused magnetic pulses to stimulate an area of the brain involved in mood regulation. It's non-invasive: no anesthesia, no sedation, nothing swallowed or injected. Your teen sits in a chair, stays fully awake and alert, and can go straight back to school or activities afterward. At Optimum, TMS is delivered with a Deep TMS system that uses a cushioned coil worn like a cap. One point of confusion worth clearing up early: TMS is not ECT (electroconvulsive therapy). They're different treatments, and the memory-and-anesthesia concerns people associate with ECT don't apply here. Because TMS isn't a medication, it also doesn't carry the whole-body side effects that come with antidepressants. "Cleared," not "approved" - and why the wording matters Most parents search for "FDA approval." For a device like TMS, the correct term is FDA clearance, not approval - that's simply how the FDA regulates this category of medical device. It isn't a lesser status or a loophole. It means the FDA reviewed the device and its evidence and determined it's safe and effective for its intended use. Here's the part that matters most for families: TMS is cleared for adolescents with depression as an add-on to standard care - meaning it's used alongside therapy and, where relevant, medication, rather than as a first thing to try before anything else. Understanding it as an add-on, not a replacement, sets the right expectation going in. Is TMS safe for teenagers? For most teens, the side effects are mild and short-lived. The common ones are a tapping sensation or some scalp discomfort at the treatment site and a mild headache, usually early in the course and easing as they get used to it. TMS doesn't sedate, and it isn't associated with the memory effects people sometimes worry about. The rare serious risk families should be aware of is a seizure, which is very uncommon. This is exactly why screening exists: before treatment starts, a clinician reviews your teen's history to identify anyone for whom TMS wouldn't be appropriate, and the team monitors throughout the course. Individual responses vary, and a good consultation will be honest with you about that rather than promising an outcome.
Quick Answer: TMS is an established, non-drug treatment for depression, and many veterans living with PTSD also carry treatment-resistant depression that TMS can address. For PTSD itself, TMS is used off-label — the evidence is promising but still developing - so whether it's a fit is decided case by case in a consultation. This guide explains where TMS stands for veterans, what the treatment involves, and how coverage typically works. Veterans coming out of therapy and medication without enough relief often start looking at what else is out there, and TMS comes up quickly. It's worth being straight about where it fits. TMS has a strong, established role in treating depression — including the depression that so frequently accompanies PTSD - and a more limited, off-label role in treating PTSD directly. This post lays out that distinction honestly, because getting it right is what makes TMS genuinely useful rather than oversold. What TMS is TMS (transcranial magnetic stimulation) uses focused magnetic pulses to stimulate a region of the brain involved in mood regulation. It's non-invasive and drug-free: no anesthesia, no sedation, nothing swallowed or injected. You sit in a chair, stay fully awake, and return to your day right after - no downtime. Because it isn't a medication, TMS doesn't carry the systemic side effects veterans often struggle with on antidepressants, and it isn't ECT - the memory and anesthesia concerns tied to ECT don't apply here. Is TMS Right for Me? Where TMS stands for PTSD - the honest version This is the part that matters most, especially if you're a provider considering a referral. TMS is FDA-cleared for depression, not for PTSD. Its use for PTSD specifically is off-label - meaning a clinician may determine it's a reasonable option based on the individual, but it isn't a formally cleared indication, and the research, while promising, is still developing. Anyone telling you TMS is a proven, approved PTSD cure is getting ahead of the evidence. Here's why TMS is still highly relevant for veterans anyway: PTSD and depression very commonly occur together. A large share of veterans with PTSD also meet criteria for major depressive disorder, and treatment-resistant depression is exactly what TMS is established and cleared to treat. So for many veterans, TMS addresses the depression side of the picture on solid, evidence-backed footing — while any role in targeting PTSD symptoms directly is handled as the off-label, case-by-case decision it actually is. That distinction isn't a technicality. It's the difference between a treatment plan grounded in what the evidence supports and one that overpromises. Why veterans consider TMS Veterans often arrive at TMS after a familiar road: multiple medications, therapy, and still not enough relief - or side effects from medication that are hard to live with. TMS offers a different mechanism entirely, which is part of why it's worth considering when the usual options haven't landed. For someone carrying both PTSD and depression , the appeal is direct: a drug-free treatment that targets the depression head-on, without adding another medication to the mix. What a course of treatment involves TMS is delivered in short, in-office sessions on a repeating schedule over several weeks. You stay awake and alert the whole time, can listen to music or relax during the session, and drive yourself home afterward. There's no recovery period. The main commitment is consistency - the schedule is part of what makes it work, so it helps to plan sessions into your week. The clinic will work with you on timing.
Quick Answer: Accelerated TMS delivers a full course of TMS in a condensed schedule - multiple sessions a day over a handful of days, instead of daily visits spread across several weeks. It suits people who can't commit to a six-week schedule or who want a faster timeline, and it's a self-pay package rather than an insurance-billed treatment. Whether it's a fit is decided in a consultation. Standard TMS works, but it asks for a real commitment: a session a day, five days a week, for around six weeks. For some people, that schedule is the problem - not the treatment. Accelerated TMS compresses the same idea into a much shorter window. This covers who it tends to suit, what the days actually look like, and the practical things to sort out before you start. What "accelerated" actually means In standard TMS, you come in once a day over roughly six weeks . Accelerated TMS keeps the treatment but changes the timetable: you receive several sessions per day, spaced out with breaks between them, across a small number of consecutive days. The result is that a course which normally spans weeks is delivered in a matter of days. It's the same underlying treatment - focused magnetic pulses to a region of the brain involved in mood regulation, non-invasive, no anesthesia, no sedation. What changes is how it's packaged into your calendar, not what it does. Who accelerated TMS is for Accelerated TMS tends to suit a specific kind of person: People who can't do six weeks of daily visits. Work schedules, caregiving, or a job that doesn't allow a daily mid-day appointment for a month and a half. Out-of-town patients. If you're traveling to Columbus for treatment, a few concentrated days is far more workable than relocating for six weeks. People who want a shorter timeline. Some patients simply want the course done sooner rather than stretched out. It's worth being straight about the flip side: the condensed schedule means several intensive days back to back, and it's a self-pay treatment rather than one billed to insurance. It's a fit for some people and not others, which is exactly what the consultation is there to sort out. Is TMS Right for You? Who it may not suit Accelerated TMS isn't automatically the better choice just because it's faster. If your schedule comfortably allows daily visits, standard insurance-covered TMS may make more sense financially, since accelerated TMS is self-pay. And as with any TMS, candidacy depends on your history and a clinical screening - the accelerated schedule doesn't change who is and isn't an appropriate candidate. That determination is made by the clinician, not by a preference for speed.
Quick Answer: TMS, Spravato, and IV ketamine are all options when standard antidepressants haven't worked well enough, but they differ in three ways that matter to most people: how they're delivered, their FDA status, and whether insurance covers them. Most major insurance plans typically cover TMS and Spravato; IV ketamine is self-pay only at Optimum. Which one fits you depends on your treatment history, your insurance, and a clinical evaluation - not on which one sounds most impressive online. If you've tried one or more antidepressants and still aren't where you want to be, you've probably come across all three of these names. They get lumped together as "advanced" or "alternative" depression treatments, which makes it hard to tell them apart. They're actually quite different from each other. This post breaks down what each one is, how the FDA classifies them, what they cost, and the kind of person each tends to suit. What each treatment actually is TMS (transcranial magnetic stimulation) is a non-drug treatment. You sit in a chair while a device delivers magnetic pulses to a targeted area of the brain involved in mood regulation. There's no medication, no sedation, and no recovery time - you drive yourself home and go about your day. Optimum delivers TMS using BrainsWay Deep TMS and NeuroStar systems. Spravato (esketamine) is a prescription nasal spray . Esketamine is closely related to ketamine, but Spravato is a specific FDA-approved formulation you self-administer in the clinic under supervision. You stay for a monitoring period afterward and can't drive yourself home. IV ketamine is ketamine delivered as a monitored infusion in the clinic . It's the same core compound that Spravato is derived from. Still, it's given intravenously rather than as a nasal spray, and it's used off-label for depression rather than under a depression-specific FDA approval. Like Spravato, it requires in-office monitoring and a ride home afterward. The FDA status is not the same for all three, and it affects coverage This is the distinction most comparison pages blur, so it's worth being precise. TMS is FDA-cleared for major depressive disorder and certain other conditions. "Cleared" is the correct term for a medical device. Spravato is FDA-approved for treatment-resistant depression. "Approved" is the correct term for a medication. IV ketamine is not FDA-approved for depression. Ketamine is FDA-approved as an anesthetic, and clinicians can prescribe it off-label for mood conditions, but it does not carry a depression-specific approval. That last point isn't a knock against IV ketamine - off-label use is legal, common, and clinically established. But it's the direct reason for the cost difference below, so it's important to understand rather than gloss over.

Quick Answer: IV ketamine therapy is a monitored, in-office infusion used to treat depression and certain other conditions that haven't responded well to standard medications . It works differently from typical antidepressants and tends to act faster, but it's used off-label, isn't covered by insurance, and requires a clinical evaluation to see if you're a candidate. This guide covers how it works, what a session is like, what it costs, and who it's for. If you've reached this page, you've probably already tried antidepressants and talk therapy without getting all the way to where you want to be. IV ketamine is one of the options clinicians turn to in that situation. It gets talked about a lot online, often with more hype than detail, so this guide sticks to what it actually is and what to expect. What is IV ketamine therapy Ketamine is a medication that's been used safely in hospitals as an anesthetic for decades. At lower doses than those used in surgery, it has shown promise for treating mood conditions, and that's how it's used here: as a controlled infusion delivered through an IV while you're monitored by clinical staff. It's important to be clear about one thing up front. Ketamine is FDA-approved as an anesthetic, but it is not FDA-approved specifically for depression. When it's used for depression, that's an off-label use - which is legal, established, and common in psychiatry, but different from a depression-specific approval. (Spravato, a related nasal-spray medication, does carry that approval; you can read how the two compare in our IV Ketamine vs. Spravato vs. TMS guide.) How it works Most common antidepressants act on serotonin and can take weeks to build up before you feel anything. Ketamine works through a different pathway in the brain - the glutamate system - and is thought to help support new connections between brain cells. That different mechanism is why many people notice changes on a faster timeline than they would with a standard antidepressant. Individual responses vary, and ketamine isn't a cure or a one-time fix. For most people, it's part of a broader treatment plan rather than a standalone solution.

Quick Answer: The "TMS dip" is a term patients use for a stretch during a TMS course where they feel worse - flatter, more tired, or more emotionally raw - before they start improving. It's widely discussed in patient communities, but it isn't a formally defined clinical event, it doesn't happen to everyone, and it isn't a required part of getting better. Most importantly: a mild rough patch is different from a significant worsening of your mood, and the second one is something to tell your care team about right away, not wait out. If you're partway through TMS and feeling worse instead of better, searching for answers at 11pm, that's an understandable place to be. The "dip" gets talked about a lot online, sometimes in ways that are reassuring and sometimes in ways that make it sound inevitable or even necessary. Neither is quite right. Here's a straight account of what people mean, what's actually known, and - the part that matters most - how to tell a normal rough patch from something you shouldn't sit on. What people mean by the "TMS dip" The phrase comes from patients, not from a textbook. It usually describes a period, often somewhere in the first few weeks of a TMS course, where someone feels temporarily worse: lower mood, more fatigue, more irritability, or a sense of being emotionally "stirred up." For people who experience it and then improve, it can look in hindsight like a dip before an upswing - hence the name. It's worth being clear that this is patient-community language. You'll see it on forums and in support groups far more than in clinical literature. Is TMS Right For You? Is the TMS dip real, and is it expected? Two honest answers here. First, plenty of people describe something like it, so it's not imaginary. Mood during any depression treatment can fluctuate, and a temporary rough stretch is a real experience for some patients. Second - and this is the part the internet often gets wrong - it is not a well-established, well-studied clinical phenomenon, and it is not something you're supposed to go through. Formal research on a defined "TMS dip" is limited. Many people complete a full course without ever feeling worse along the way. So if you're not experiencing it, nothing is wrong; and if you are, it doesn't mean you're on some required path that everyone walks. Be skeptical of anyone - online or otherwise - who tells you that feeling worse is a sign the treatment is working. That's not a reliable rule, and treating it as one can lead people to ignore a genuine downturn.

Quick Answer: After the monitored observation period at the clinic, you'll head home with a driver - you can't drive for the rest of the day. It's normal to feel tired, foggy, or a little "off" for a few hours, with most of those effects fading by the time you wake up the next morning. Don't read too much into how you feel emotionally after one session; Spravato's effect is tracked over a course of treatment, not judged on day one. Here's what the rest of your day, the next morning, and the weeks ahead typically look like. You've had your first Spravato (esketamine) session , sat through the observation period, and now you're heading home, wondering what the rest of the day holds. This post picks up right there. If you haven't had your first appointment yet and want to know what happens during the session, start with What to Expect at Your First Spravato Session - this guide is about everything that comes after. The rest of your first day The most important practical point: you cannot drive after a Spravato session. That's why you arranged a ride, and it's a firm rule, not a suggestion. Plan to be a passenger for the rest of the day. Once you're home, the best thing you can do is take it easy. Many people feel drained, spacey, or mildly dreamy for a few hours after the dose as the medication's effects wind down. Some feel more or less normal fairly quickly. Both are within the range of typical. A quiet evening - no big plans, no demanding tasks - is the right call. What you might feel in the hours afterward During the session you may have noticed a floating or detached feeling. As the afternoon goes on, that generally continues to fade. In the hours after, some people experience: Tiredness or a wish to nap Lingering mild dizziness or unsteadiness A slightly foggy or slowed-down feeling Mild nausea These tend to be short-lived and ease as the medication clears. The clinic monitors things like blood pressure during your observation period specifically, so you leave when it's appropriate, which is part of why the in-office monitoring exists. If something feels more intense or lasts longer than you expected, that's worth a call to the clinic rather than something to tough out alone.









